Adenomyosis: Ultrasound & MRI Findings Explained
Could a hidden condition be the source of your chronic pelvic pain and heavy periods? Adenomyosis, a often-overlooked gynecological condition, affects many women, often leading to significant suffering and is sometimes misdiagnosed or undiagnosed for years.
The complexities of women's health often present diagnostic challenges, and conditions like adenomyosis exemplify this. This is a common benign uterine condition where endometrial tissue, which normally lines the uterus, grows into the muscular wall of the uterus (myometrium). This ectopic endometrial tissue can cause a variety of symptoms, ranging from painful periods (dysmenorrhea) and heavy or prolonged menstrual bleeding (menorrhagia) to chronic pelvic pain and, in some cases, infertility. While it is a benign condition, adenomyosis can significantly impact a womans quality of life.
Adenomyosis classically affects multiparous women of reproductive age, but it's important to remember that any woman can be affected. Its diagnosis can be tricky, as symptoms can overlap with other conditions like endometriosis or fibroids. Furthermore, up to a third of patients may be asymptomatic, making detection even more challenging. The condition's variable presentation and the lack of consistent awareness contribute to delayed diagnosis and treatment.
The diagnosis of adenomyosis relies heavily on imaging techniques. Ultrasound, and particularly transvaginal ultrasound (TVUS), is typically the first-line imaging modality. Magnetic Resonance Imaging (MRI) can also be used, and both can show characteristic findings that can help to identify the condition. Technological advancements in ultrasound have led to increased diagnostic capabilities. The morphological uterus sonographic assessment (MUSA) consensus statement provides valuable guidance on how to describe typical adenomyosis imaging features using ultrasound. However, there's still a lack of standardized consensus for descriptors and subtypes when it comes to MRI.
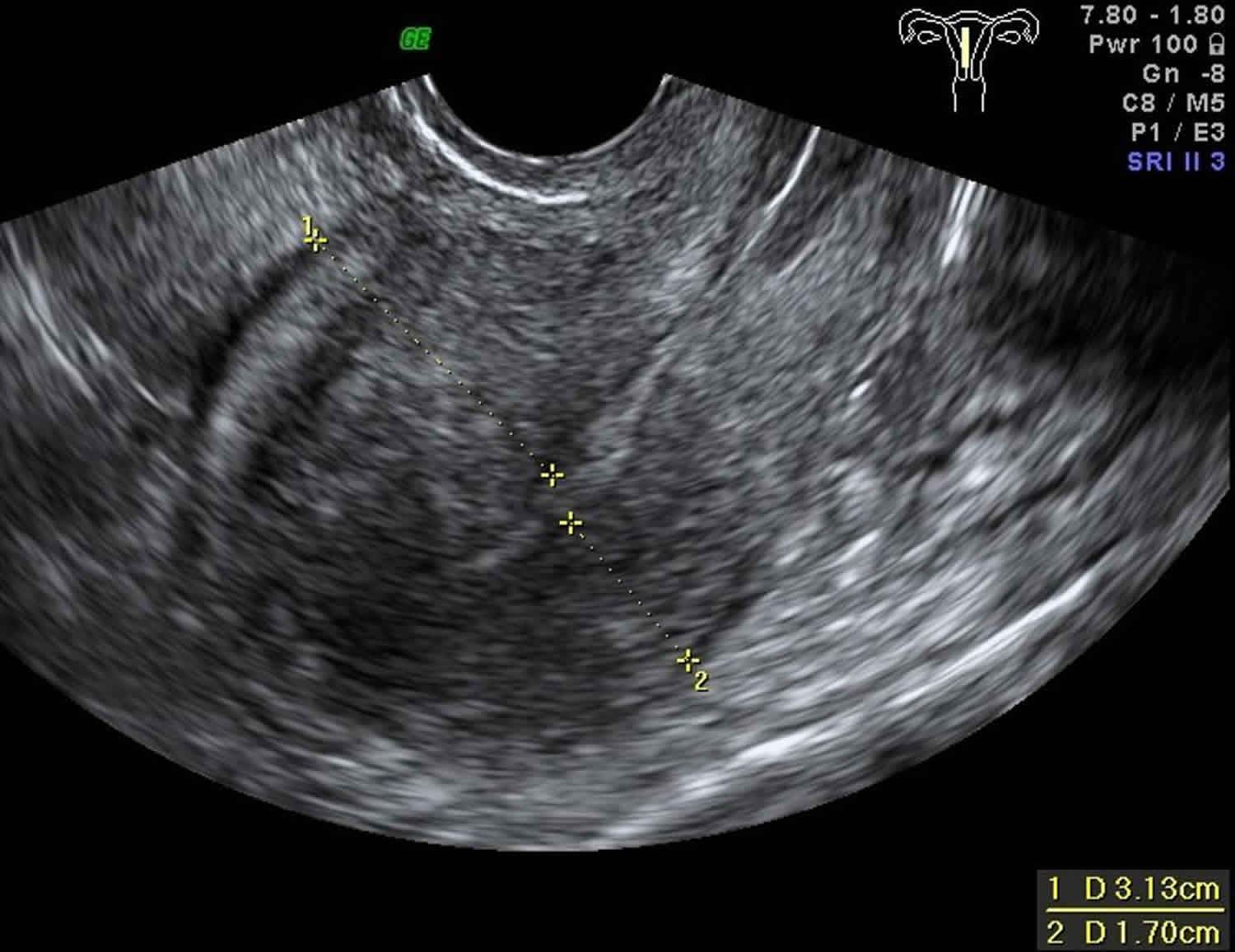
On ultrasound, adenomyosis often presents with features like focal or diffuse myometrial bulkiness, which may be asymmetrical, and a heterogeneous myometrium. Other features include asymmetrical uterine wall thickening, increased blood flow, and the "venetian blind" pattern of acoustic shadowing. The "question mark sign", visible on ultrasound images of a retroverted uterus with adenomyosis, is a classic visual indicator. Power Doppler imaging can also reveal diffusely spread small vessels within the uterine wall.
A pelvic examination may reveal an enlarged uterus, and that might be tender when touched. Diagnosis can be confirmed via the use of Magnetic Resonance Imaging (MRI) or Ultrasound, which provide detailed images of the uterus. Unlike fibroids, which typically appear as discrete masses within the uterus, adenomyosis is characterized by diffuse involvement of the uterine wall. Ultrasound can also help distinguish adenomyosis from other conditions, such as endometrial polyps, which appear as focal outgrowths from the uterine lining.
Transvaginal ultrasound (TVUS) is the primary imaging method for the diagnosis of adenomyosis, and radiologists are well-versed in its sonographic appearance. Transvaginal ultrasound is reported to be as sensitive (89%) and specific (89%) as MRI in diagnosing uterine adenomyosis.
The most common ultrasound features of adenomyosis include asymmetrical myometrial thickening, transitional zone thickening >12 mm, heterogeneous myometrial echopattern, and myometrial echogenic linear or nodular striations.
| Feature | Description |
|---|---|
| Common Features |
|
| Ultrasound Findings |
|
| Other Related Information |
|
For further information, consider consulting resources like the Mayo Clinic
The invasion of endometrial glands and stroma into the myometrium is a key characteristic of adenomyosis. This condition is also linked to smooth muscle hyperplasia and fibrosis within the uterine wall. This invasive process causes the myometrium to respond, leading to thickening, inflammation, and pain. Dysmenorrhea (painful periods) is often a leading complaint, often worsening over time, as the condition progresses. Heavy menstrual bleeding (menorrhagia) is another common symptom that results from the compromised integrity of the uterine lining.
The presentation of adenomyosis can differ among women. Some may be asymptomatic, especially in the early stages of the condition, which contributes to diagnostic delays. Others experience mild symptoms that are often dismissed or attributed to other causes. Still, many women report significant pelvic pain, which can include chronic pain between periods, pain during sex (dyspareunia), or other related symptoms. This variability makes diagnosis a challenge, and it is vital for healthcare providers to maintain a high degree of suspicion when evaluating patients with related symptoms.
In the diagnostic process, a detailed medical history, including a review of symptoms, menstrual patterns, and family history, is critical. A physical examination, including a pelvic exam, can provide clues, and imaging studies, primarily ultrasound, are often crucial for visualizing the uterus and identifying characteristic features. MRI can also provide detailed information.
The clinical significance of adenomyosis spans beyond the immediate symptoms. The pain and bleeding it causes can significantly affect a womans quality of life, impacting her ability to work, socialize, and maintain relationships. Adenomyosis can also negatively affect fertility and pregnancy outcomes. Women with adenomyosis may experience difficulty conceiving, and are at increased risk of miscarriage, preterm labor, and other pregnancy complications. Addressing adenomyosis can be a vital step in helping women achieve their reproductive goals.
Management of adenomyosis involves a tailored approach based on the severity of symptoms, the patients reproductive goals, and overall health. Treatment options range from conservative measures, such as pain medication and hormonal therapies, to surgical interventions. Nonsteroidal anti-inflammatory drugs (NSAIDs) can help to reduce pain and inflammation. Hormonal treatments, including oral contraceptives, hormonal IUDs, and gonadotropin-releasing hormone (GnRH) agonists, can help manage symptoms by suppressing the menstrual cycle and reducing endometrial tissue growth.
For women who do not respond to medical management or who desire definitive treatment, surgical options are available. Hysterectomy, the removal of the uterus, is a definitive treatment for adenomyosis, and it eliminates the source of the problem. In certain situations, less invasive surgical procedures, such as endometrial ablation or adenomyomectomy (removal of the affected areas of the myometrium), can be considered, but these may not be suitable for everyone. The most appropriate treatment is determined by carefully assessing the individual's needs and preferences in consultation with their healthcare providers.
Recent advances in diagnostic techniques and therapeutic strategies have improved outcomes for women with adenomyosis. Ongoing research aims to better understand the underlying mechanisms of the condition and to develop more effective and less invasive treatment options. Early diagnosis and prompt intervention play a key role in the overall care of patients.
The use of ultrasound in diagnosing adenomyosis continues to evolve. 3D ultrasound and Doppler techniques provide more detailed images. These improvements increase the accuracy of the diagnosis. The MUSA consensus statement provides a standardized approach for describing the sonographic appearance of adenomyosis, helping to make diagnosis more consistent.
The international morphological uterus sonographic assessment group published in 2015 a consensus on terminology to use when describing myometrial lesions seen on ultrasonography [1 2]. Further research is needed to refine the diagnostic criteria and to evaluate the effectiveness of different treatment modalities. This research includes investigation of new imaging techniques and minimally invasive surgical procedures.
In order to differentiate clinically suspected cases of leiomyoma and adenomyosis of the uterus, Sharma k, bora mk, venkatesh bp, barman p, roy sk, jayagurunathan u, et al. conducted research on the role of 3d ultrasound and Doppler. Adenomyosis is a common gynecologic disease characterized by the invasion of endometrial glands and stroma into the myometrium and is associated with smooth muscle hyperplasia and fibrosis. Adenomyosis (or uterine adenomyosis) is a common uterine condition of ectopic endometrial tissue in the myometrium, sometimes considered a spectrum of endometriosis. Although most commonly asymptomatic, it may present with menorrhagia and dysmenorrhoea. In the cases of septate uterus, the septum is seen merging with the myometrium above in the fundus.
In summary, adenomyosis is a complex condition requiring careful evaluation and management. Increased awareness, early diagnosis, and the right treatment approach can significantly improve the health and quality of life for women dealing with the condition.


Detail Author:
- Name : Margret Schamberger
- Username : demetris.renner
- Email : otis.lubowitz@walter.com
- Birthdate : 2001-11-25
- Address : 6332 Casper Vista Suite 976 Donatoview, MT 13894-7494
- Phone : 351-678-7474
- Company : Erdman and Sons
- Job : Substance Abuse Social Worker
- Bio : Qui illo molestiae et esse. Expedita facilis voluptatem temporibus quae sapiente facere officia. Consequatur ipsam et fugiat et. Corporis itaque aliquam reprehenderit in culpa eos quia.
Socials
linkedin:
- url : https://linkedin.com/in/mosciskil
- username : mosciskil
- bio : Assumenda nulla tenetur illo sit.
- followers : 3349
- following : 2077
facebook:
- url : https://facebook.com/lonie5181
- username : lonie5181
- bio : Eveniet ut nisi eum non. Neque qui repudiandae quis dolor.
- followers : 3227
- following : 411
tiktok:
- url : https://tiktok.com/@mosciskil
- username : mosciskil
- bio : Qui et eum impedit similique ipsam natus. Adipisci in nihil fuga vel.
- followers : 4629
- following : 831


{kind=link}